Consultation
Vitrectomy
Eye Conditions
Cataract
CSCR
Diabetic Retinopathy
Epiretinal Membrane
Flashes and Floaters
Glaucoma
Macular Degeneration
Macular Hole
Retinal Detachment
Retinal Vein Occlusion
Uveitis
Vitreomacular Traction
Investigations
Procedures
Vitrectomy is a surgical technique to remove the vitreous gel. The vitreous fills the eye cavity between the lens and retina. Because the vitreous contains collagen fibres, it cannot simply be sucked out. An automated cutter at the tip of a fine needle-like instrument is used to cut and suck out the vitreous.
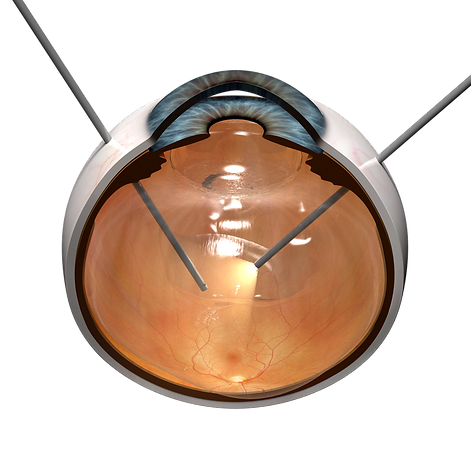
Modern vitrectomy is performed through three small wounds in the sclera (the white of the eye), which are constructed so that they self-seal. Stitching is therefore usually not needed. One wound is used to keep the eye pressurised with infusion of fluid, which replaces the vitreous removed through the cutter. The other two wounds are used for the light illumination and vitrectomy cutter. The surgeon sees the interior of the eye through dilated pupil using a complex set of lenses attached to the operating microscope.
Conditions treated by vitrectomy include:
-
Vitreous haemorrhage, e.g., from severe diabetic retinopathy
-
Macular disorders: Macular hole, epiretinal membrane, vitreomacular traction
-
Trauma, especially with intraocular foreign body
Vitrectomy performed using small wounds is safe, quick and painless, with the patient making a rapid recovery. Some irritation after the surgery is expected but severe discomfort is unusual. Recovery of vision depends on the condition treated, as well as whether gas or silicone oil is infused in the eye cavity to support the retina. The gas resolves spontaneously over a number of weeks, which will be apparent as an undulating line that gradually moves down. The vision will be clearer above this line. The line turns into an arc, becoming a dark blob at the bottom that eventually disappears. Airplane travel is absolutely prohibited while gas is in the eye. Silicone oil needs to be removed through a second surgery, when the retina is confirmed to be stable.
A significant disadvantage of vitrectomy is that it will accelerate cataract formation. Most conditions treated by vitrectomy pose a threat of permanent vision loss, justifying the need for a second procedure to optimise vision later on. If there is significant cataract already, vitrectomy can be combined with cataract surgery.